The Stability Framework
The Stability Framework is a three-phase sequencing architecture for withdrawal stabilization and dose reduction from kratom, 7-hydroxymitragynine (7-OH), Suboxone and opioid dependence — built on the principle that system stability must precede reduction, and that the order of operations determines whether a taper holds or collapses.
The Stability Framework is designed for dependence patterns where the primary need is stabilization before reduction. For individuals in a compression cycle pattern — dosing multiple times daily — the Kinetic Bridge may be the more appropriate starting point. The Quit Plan Builder will assess your pattern and route you to the right next step.
Most people searching for a way off kratom or Suboxone are looking for a schedule. How much to cut, and when.
The Stability Framework is something different. It is a sequencing model — built on the principle that the order of operations matters more than the pace of reduction. Stabilize the system first. Then reduce inside stability.
That sequence is not intuitive. It feels like a delay. It isn't. It's the difference between a taper that holds and one that collapses in the same place it's collapsed before.
Why Reduction Keeps Failing
The nervous system adapts to whatever it lives inside.
When kratom or Suboxone has been part of daily function long enough, the system stops treating it as something external and starts building around it. Sleep anchors to dosing timing. Mood organizes around the relief signal. The interval between doses becomes the operational unit the nervous system tracks.
When reduction is attempted inside this adapted state, the system doesn't interpret it as progress. It interprets it as a threat. Sleep fragments. Urge pressure increases. The interval compresses. The taper that looked manageable on paper stops being manageable by day three.
This is mechanical, not motivational. The Volatility Density Index (VDI) measures this state across five domains — sleep continuity, dosing intervals, urge pressure, redosing behavior, and emotional regulation. When volatility is elevated across those domains, reduction amplifies instability rather than resolving it. The VDI doesn't measure dose. It measures the conditions that determine whether a reduction will hold.
The Emotional Dimension
One thing most people don't expect — and don't have language for until they see it named: the emotional dimension of withdrawal from kratom and high-potency products is not secondary to the physical picture. It is equal architecture.
The mu-opioid system is a primary regulator of mood, stress response, and the capacity to process difficulty. When kratom alkaloids and 7-OH clear between doses, that regulatory function clears with them. What follows is not random. It is predictable — waves of dysphoria, grief, anxiety, and flatness that arrive on the dosing schedule and lift when the dose lands.
If the emotional drops arrive reliably between doses and resolve reliably when the dose lands — that's not a mood disorder. That's the mu-opioid system's emotional regulatory function cycling with the pharmacokinetics. The schedule is the evidence.
This is G-protein Biased Autonomic Dysregulation (GBAD) — a withdrawal presentation that standard clinical tools weren't designed to capture, and that most people have been trying to manage without a name for it. Understanding it changes how stabilization is sequenced and why emotional stability has to be part of the target, not just a byproduct.
Sleep Is the Signal
Sleep continuity is where instability shows up first. Before cravings intensify, before function deteriorates — sleep starts to fragment. Waking at 3 AM. Shallow hours. Running depleted by afternoon.
Sleep is the earliest signal that the system is unstable and the last signal to fully resolve. When sleep breaks during a taper, the reduction moved faster than the nervous system could track. Protecting sleep is not optional. It is the primary stability marker the entire framework is built around.
Pattern Trajectory
A VDI score tells you where the system is. Pattern Trajectory tells you where it's heading.
A person with a moderate score whose pattern is stabilizing is in a fundamentally different position than someone with the same score whose pattern is tightening. The direction matters as much as the number. Reductions that begin while the trajectory is still tightening almost always fail — not because the score was wrong, but because the system was still accelerating when the attempt began.
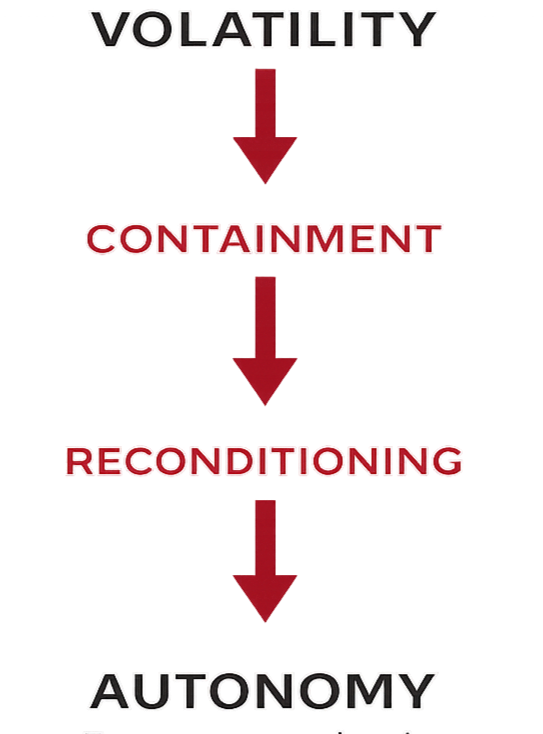
The Three Phases
The Stability Framework organizes the stabilization and reduction sequence into three phases.
Containment
Before any reduction occurs, the pattern must be stabilized. Containment means establishing predictable dosing intervals, eliminating preventative redosing, protecting sleep timing, and reducing environmental stress load. These elements restore rhythm to a nervous system that has been organizing itself around managing the next episode.
This phase often produces the first real signs of forward movement — longer sleep intervals, reduced emotional amplitude, less urgency between doses. Sleep continuity is the clearest signal that containment is working.
Reconditioning
Once instability decreases, the nervous system begins adapting to a new baseline. Reconditioning involves gradual interval extension, structured reductions when stability markers permit, and rebuilding the system's tolerance for normal stress and routine.
Reductions that would have triggered collapse during the volatile phase become manageable here — because the system now has margin to absorb change.
Autonomy
Autonomy represents the return of stable self-regulation. Sleep consolidates. Emotional amplitude decreases. Urges lose their urgency. Use intervals extend without pressure.
The goal is not simply cessation. It is a nervous system that regulates itself again.
What Comes After
The exit is not the finish line.
The Persistent Pathway names what happens to the reward system after prolonged use. Receptor changes don't clear when the substance does. Recovery feels flatter and longer than expected — not because something is wrong, but because the system is rebuilding infrastructure that was meaningfully reorganized. Understanding that mechanism changes how people interpret the post-exit window and what inputs actually accelerate recovery.
The Deeper Framework
The concepts that underpin this framework — CCOD, GBAD, the Pharmacologic Cycle Overwrite, Activation Slope Induction, Retail Pharmacology — are documented in full on the Core Concepts page. These are original frameworks developed within Pivot Protocols to address patterns the existing clinical literature had not yet formally named.
Where to Start
The Quit Plan Builder assesses your current stability pattern across the VDI domains and routes you to the right next step. Thirty seconds. No email required.
Build Your Quit Plan →
For clinicians and researchers: The Stability Framework is a sequencing model for behavioral stabilization before dose reduction — organizing the containment, reconditioning, and autonomy phases that govern successful taper progression in this population. The terminology is new. The mechanisms are not. For Professionals →
John Leonard is the founder of Pivot Protocols and a recovery program leader with 23 years of front-line experience. The frameworks on this site were developed through direct observation, pattern recognition, and grounding in published pharmacological research. He is not a clinician or medical provider.
This framework is offered for educational purposes only. All clinical decisions are made solely between the patient and their licensed medical provider.